|
|

|
Nuclear Medicine Imaging:
Other Prostheses & Physiologic States
by Gagandeep Choudhary, MD and Phillip Kuo, MD, PhD
Miscellaneous Medical Conditions and Surgical Artifacts
Focal bone marrow uptake may simulate bone infection, especially if it is an unusual location or situated next to an orthopedic prosthesis that could have associated loosening or infection (figure 32). Heterotopic bone formation (also called myositis ossificans) is fairly common after muscle injury or surgery of the extremities and joints. It can be seen in both the upper and lower extremities. It is particularly common in the elbow and hip after surgery or immobilization. It may be quite prominent and bizarre in its early stage and can be confused with malignancy if one is not careful. It is most easily recognized on hip, femur, or pelvis radiographs but is often seen on other imaging studies (figure 33). It is a benign finding that usually needs no further evaluation or treatment.
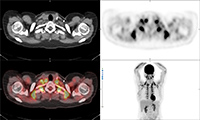
Brown fat or brown adipose tissue (BAT) and white adipose tissue are the two kinds of fat (adipose tissue) found in mammals. Brown fat is especially abundant in newborns with its primary function being to generate body heat. Brown fat cells contain many small droplets of lipids and a high number of mitochondria which make it brown. It contains more capillaries than white fat having a greater need for oxygen delivery. Brown fat becomes less common as one ages. It is still present in adults in the upper chest, neck, paraspinal, and suprarenal regions and is more metabolically active with cold exposure (figure 34).
Surgical fixation apparatus - plates, screws, cages, rods, nails, prosthesis - most commonly cause signal loss and photopenia on nuclear medicine studies from their absorption or scatter of radiotracer photons originating deeper in the body. Sometimes, they may stimulate bony healing or bony reaction with an increase in radiotracer signal (figure 35).
Conclusions
Nuclear medicine produces exquisite physiologic imaging of various organ systems depending on the radiopharmaceuticals and imaging equipment used. Nuclear medicine images are primarily functional. Artifacts caused by objects in or on the body cause more morphologic than physiologic change. They should not interfere with interpretation if they are properly recognized, and if the nuclear medicine images are closely correlated with the patient's other imaging studies and clinical picture.
Normal physiologic processes and pathologic processes are often incidentally noted on nuclear medicine imaging done for other purposes. Their appearance can be quite bizarre. Fortunately, they follow set patterns and principles leading to their recognition if one is experienced and has access to the patient's clinical history, laboratory results, and imaging studies. This article is a brief review of some of the artifacts found on nuclear medicine studies with an emphasis on orthopedic apparatus. Artifacts abound in all types of imaging and new artifacts will surely appear as imaging systems become more complex (Patton, 1994).
Back to Top
| Figure 29 |
Figure 30A |
Figure30B |
Figure 30C |
 |
 |
 |
 |
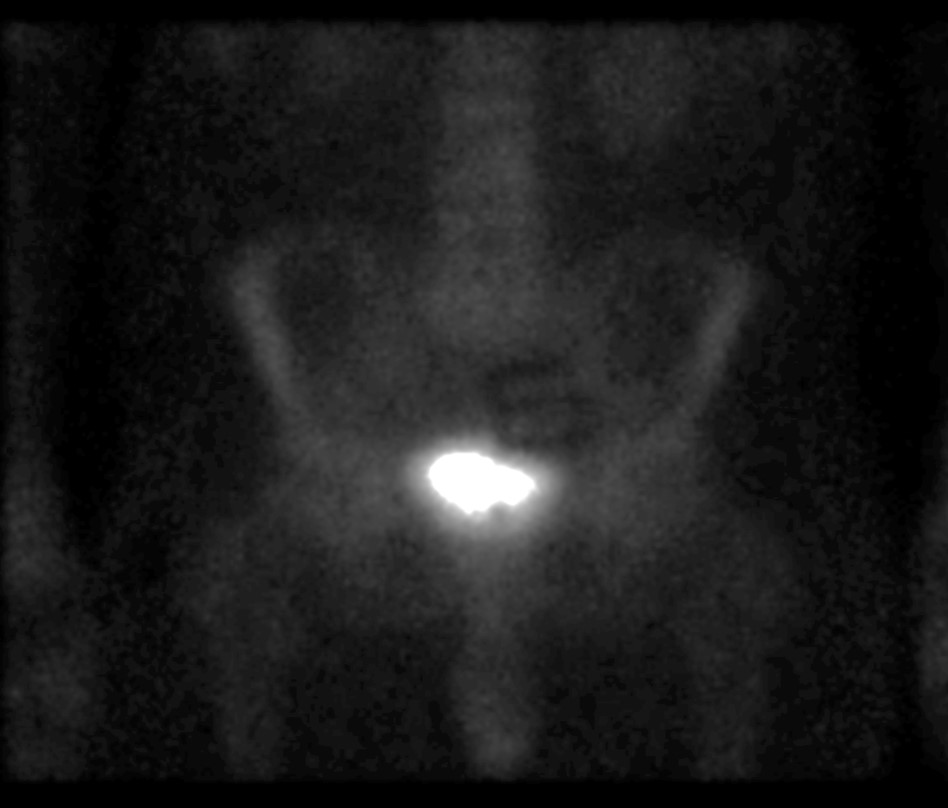
| Thyroid imaging with pinhole collimator after the injection of free Tc-99m pertechnetate shows a rounded focal photopenic defect in the region of the left lower thyroid lobe caused by a nonfunctional photomultiplier tube. |
Focal intense activity seen in the right antecubital region and along the right lateral abdominal wall on Tc-99m MDP scan is related to extravasation of radiopharmaceutical at the injection site with scatter of photons from the forearm to the abdominal wall (narrow angle scatter). |
Fused axial FDG PET-CT (B), PET axial (C), CT axial (D) and MIP PET (E) images demonstrate intensely FDG avid lymph node in the right axilla. Infiltration of FDG at the injection site in right antecubital fossa results in lymphoscintigraphy with FDG migrating to the regional nodal basin via the lymphatic ducts. |
 |
| Figure 30D |
Figure 30E |
Figure 31 |
|
 |
 |
 |
|
| Fused axial FDG PET-CT (B), PET axial (C), CT axial (D) and MIP PET (E) images, demonstrate intensely FDG avid lymph node in the right axilla. Infiltration of FDG at the injection site in right antecubital fossa results in lymphoscintigraphy with FDG migrating to the regional nodal basin via the lymphatic ducts. |
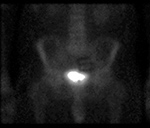
Technetium 99m MDP whole body bone scan shows photopenic defect on the midline pelvis from the attenuation of a belt buckle. |
|
|
| Figure 32A |
Figure 32B |
Figure 33 |
Figure 34 |
 |
 |
 |
 |
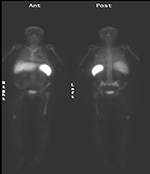
| 63 year-old woman with right femoral hardware for 3 years presented with right leg pain. Whole body Tc-99m HMPAO tagged WBC (A) scan demonstrated focal abnormal activity in the distal right femur which may represent infection or focal marrow. Tc99m sulphur colloid bone marrow scan (B) four weeks later demonstrates similar focal uptake in the distal right femur confirming the etiology as uptake in displaced marrow and not infection. |
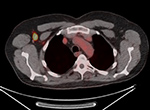
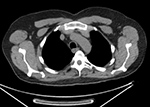
60 year-old man with history of lung cancer and left hip arthroplasty suffered from stiffness in the left hip region. Axial CT, FDG PET, fused axial, and coronal PET-CT demonstrates increased uptake of FDG in heterotopic ossification in the musculature of the left thigh. |
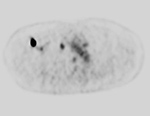
30 year-old woman with history of lymphoma. Axial CT, PET, PET-CT fused, and PET MIP images demonstrate intense FDG activity in the bilateral neck and paravertebral regions with a symmetrical distribution. Cross-sectional images clearly show that activity in the neck corresponds to fat and therefore consistent with brown fat activity. Brown fat activity is seen more commonly in younger patients and is also increased in response to hypothermia (so keep patients warm both pre and post injection of FDG). |
|
| Figure 35A |
Figure 35B |
|
|
 |
 |
|
|
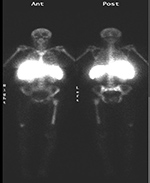
| PA Chest radiograph (A) demonstrates a sternal cage. Whole body Tc99m MDP images (B) demonstrate focal radiotracer activity in ribs bilaterally on the anterior view representing the sites of sternal cage fixation with bony reaction. |
|
|
Back to Top
|